 A recent study, published by MBJ Open Ophthalmology, set out to determine if automated OCT aids in the management of patients in a high-volume after-hours clinic.
A recent study, published by MBJ Open Ophthalmology, set out to determine if automated OCT aids in the management of patients in a high-volume after-hours clinic.
OCT has become the standard of care for diagnosing plenty of ocular pathologies, but is generally not available at most institutions after-hours -- when many patients present with acute complaints. Richard I. Kaplan, MD, New York Eye and Ear Infirmary of Mount Sinai, and his team, obtained images over a period of 15 months (202 patients, 359 eyes), reviewed electronic patient records, and surveyed staff to measure the advantages of having an automated OCT for diagnosis and management of acute complaints and ocular emergencies.
Chief complaint, image type, image findings and diagnosis were analyzed. Ultimately, patient complaints included flashes/floaters, metamorphopsia, decreased vision and scotomas. Diagnoses comprised of vascular occlusion, retinal detachment, macular hole, cystoid macular edema and central serous retinopathy.
Twenty-five residents and fellows participated in the voluntary survey. All residents (n=18) and fellows (n=7) found the OCT to be helpful; 15 residents (83%) and 4 fellows (57%) felt that it changed management. Most participants, (21 or 83%), felt that the OCT improved patient satisfaction and reduced delayed or misdiagnosis. Most participants (19 or 76%) also reported reduced physician stress.
Kaplan et al noted OCT aids in the quickly-needed diagnosis of central retinal artery occlusion (CRAO) – data showed six patients with CRAO, and OCT successfully confirmed five.
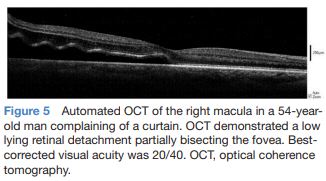
They also highlighted OCT’s use in differentiating macular-involving versus macular-sparing retinal detachment, leading urgent retinal detachment repair or surgical planning and patient couselling. “In cases of macula-off retinal detachments, the OCT provides objective documentation. As most ophthalmic lawsuits in the USA relate to RD, such documentation substantiates the appropriateness of care in the after-hours setting,” Kaplan explained.
OCT was also found helpful in ruling-out emergent pathology, thus refining triage of patients to subspecialty clinics in hospital and reducing the need for after-hours subspecialty consults. The study included 14 patients with central serous retinopathy who, in general, with OCT verification, follow-up appointments could be extended to 3 weeks.
Although trauma cases were not well represented in the sample, OCT appears to aid in the identification of globe perforation and may aid in ruling out such injuries in the emergency setting.
Finally, one limitation of automatic OCT is the minimum vision requirement necessary for patients to find fixation cues without operator redirection. Some attempted scans had insufficient signal strength, all in patients with visual acuity 20/400 or worse.
“In the after-hours or acute-care setting, the most important goal of care is the timely diagnosis and treatment of vision threatening pathology while efficiently using ancillary testing and consultants. We found OCT accessibility in the after-hours setting improved the diagnosis and disposition of patients. Additional studies will be helpful to further appreciate the benefits of including OCT alongside clinical examination in both eye-only and general emergency settings.”